
INSIDE THE ISSUE
> Total Healthcare Expenditures
> Input Costs Drive Health Costs
> Mobile Integrated Health
> Foster G. McGaw Prize
> Ruling Against Leapfrog
> Mass. Broadband Program
MONDAY REPORT
Healthcare Spending Rose Along With Everything Else
The Center for Health Information and Analysis (CHIA) has released its latest annual report on how the state’s healthcare system is performing, which found that Massachusetts’s healthcare expenditure growth in 2024 was less than the national average and compared closely to the state’s overall economic growth.
The 5.7% increase in total healthcare spending in 2023-2024 is above the 3.6% healthcare cost growth benchmark that the state sets each year. That benchmark is based on an arbitrary “potential gross state product” determination that is consistently far below actual state GDP, which is the measure that the 2012 healthcare reform law had intended healthcare spending growth to align with.
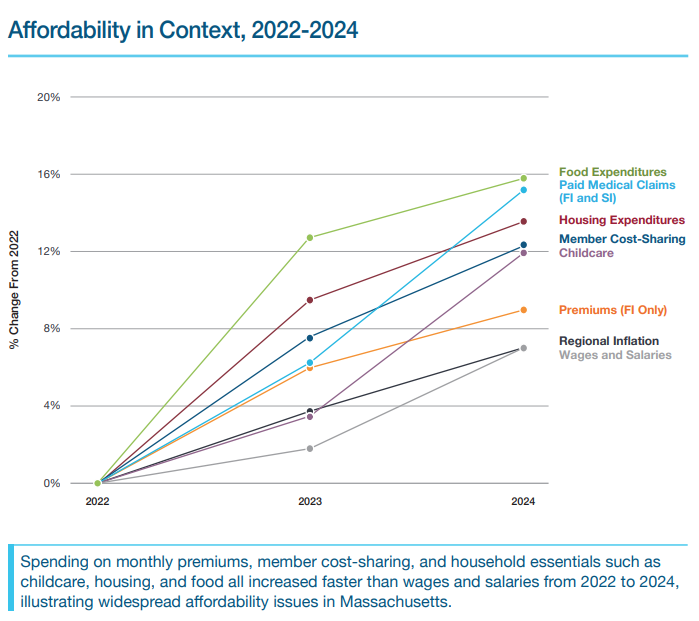
The rising cost of healthcare is part of a trend of rising costs across many sectors and overall regional inflation, according to the CHIA report. “Member cost-sharing” for healthcare rose 12.3% between 2022 and 2024, but food prices spiked 15.8% during the same time, while housing costs grew by 13.6%, and center-based childcare by 12%, according to CHIA. “Therefore, healthcare cost trends must be evaluated within the context of these broader economic circumstances,” the state agency wrote. National per-capita healthcare spending growth (6.1%) was higher than the commonwealth’s 5.7% growth, which was comparable to the state’s 5.5% GDP growth in 2024.
CHIA’s report builds on data beginning from more than two years ago in 2023 and running through the end of 2024. It covers the period when Steward Health Care collapsed, when the healthcare system was facing 17,000 workforce vacancies, and when there was a $200 million deficit in the Health Safety Net fund that covers care for uninsured and underinsured patients.
According to CHIA, the biggest driver of total healthcare expenditures (THCE) in the state was pharmacy spending, which increased by $1.1 billion or and was responsible for 23.2% of overall THCE growth between 2023 and 2024. Next was hospital outpatient services, which accounted for 21.8% of THCE growth. For the first time in its reporting, CHIA identified that 20% of that outpatient spending growth was attributable to the cost of drugs used in outpatient care.
While healthcare spending grew, hospital margins dipped into the red. The statewide median operating margin for Massachusetts hospitals was negative -2% in Hospital Fiscal Year 2024, plummeting from the 0.2% margin the year before, according to CHIA. Seventy-four percent of hospital health systems – which include affiliated physician groups – experienced negative operating margins in FY24; the statewide median operating margin was -2.4% for hospital health systems that year.
The rising healthcare expenditures translated into rising premiums for fully insured residents in employer-sponsored health plans; their premiums rose 4.8% in 2024, or an average of $683 per member per month, CHIA found.
“2024 embodied the unsustainable balance our healthcare sector now faces every day: the mission of delivering uninterrupted care through crisis and the challenge of absorbing ever-climbing input costs,” said MHA’s Senior Vice President of Healthcare Finance & Policy Dan McHale. “That’s why we’re grateful for the state’s focus on affordability and the root causes of healthcare costs – including administrative burdens and rising supply costs.” He added that “MHA echoes the call for urgent collaborative action and smart policy” to repair the state’s world-class health system.
AHA Report: Rising Input Costs Leads to Higher Health Costs
The American Hospital Association (AHA) has released a report assessing hospital costs in 2025, focusing on which factors are driving changes from prior years.
The report found that while the cost of hospital care has increased, total hospital expenses – that is, the money facilities spend on drugs, fuel, labor, and more – grew at a 7.5% rate in 2025, or more than twice the rate of growth in hospital prices over the same period. Hospital spending on drugs was four times higher than the growth in hospital prices in 2025, AHA found. The report reflects the financial pressures Massachusetts hospitals have been experiencing and which are reflected in the rise of the state’s healthcare expenditures (see story above).
“Hospitals are not only paying more to provide care, they also are delivering more care to patients who are sicker and more medically complex,” according to AHA’s Cost of Caring report. “A recent AHA/Vizient analysis found that hospital case-mix index — a standard measure of how sick patients are — rose by about 5% between 2019 and 2024, indicating that a larger share of hospital care is devoted to higher-acuity patients with multiple conditions, greater clinical needs and longer stays.”
Labor costs also grew as did incidences of “payment friction,” such as the costs involved in overturning denied claims from health insurance companies. AHA found that hospitals spent nearly $18 billion on overturning claims denials alone in 2025.
Yes, the cost of care is rising, AHA concluded, but not as fast as the expenses hospitals incur in providing that care. “In other words, despite hospitals facing higher labor and input costs, treating more patients with greater clinical complexity, and maintaining essential, always-on services that communities depend on, they have managed to keep price increases below the increases in their input costs,” AHA wrote. “However, this mismatch between expenses and revenue leaves hospitals increasingly at risk of being able to maintain the full spectrum of services on which communities rely.”
The national report is especially timely since the U.S. House’s Energy and Commerce and Ways and Means committees have been holding a series of hearings on healthcare affordability, and they plan to focus this week on provider costs.
Hospital Leaders: Help Us Keep People Out of Hospitals!
Last Wednesday a group of experts employed by and committed to Massachusetts hospitals had a clear message to a group of policymakers that met at the State House: sometimes keeping people out of hospitals is the best way to care for them.
House Chair of the Joint Committee on Health Care Financing John Lawn (D-Watertown), joined by House Chair of the Joint Committee on Cannabis Policy Dan Donahue (D-Worcester), and House Chair of the Joint Committee on Bonding, Capital Expenditures, and State Assets Mike Finn (D-West Springfield) hosted last week’s briefing on hospital at home (HAH) and mobile integrated health (MIH) programs. They were joined by representatives from MHA, UMass Memorial Health, Mass General Brigham, and Lowell General Hospital.
Hospital at Home programs allow patients to receive acute-level inpatient care in the comfort of their own home. Mobile Integrated Health allows providers to leverage mobile resources, including EMS, to deliver ongoing care to patients in a personalized environment outside of healthcare facilities. Currently, Medicare and MassHealth reimburse for HAH services, but commercial plans do not. Insurers also do not cover MIH programs. Two bills now pending at the State House would provide coverage and reimbursement for the programs, allowing them to be sustainable and grow in the future.
At the briefing, UMass Memorial Health’s President & CEO Eric Dickson, M.D., a member of the MHA Board of Trustees, said his long experience with HAH and MIH, as well as the numerous scholarly studies on the programs, demonstrate clearly and convincingly that they work in improving outcomes, lowering costs, and keeping patients and families happy to be care for in familiar surroundings.

Keeping non-emergent cases out of the ED, the most expensive care site in the health ecosystem, has been a longtime goal of policymakers. Anyone calling 911 will be transported to an ED, which can entail thousands of dollars for an ambulance ride, thousands more for the ED visit, tens of thousands for a hospital admission, and tens of thousands more for subsequent care at a skilled nursing facility (SNF), Dickson said.
“Think of that cascade,” Dickson said. “The question is can we break that cascade? Can we keep people in their home when they deteriorate? … And the answer that I can say with absolute certainty today, with scientific papers to back me up, is that it works.” Monitoring people remotely, sending an EMT to a person’s home (in a car not an ambulance) when they need it, and doing daily check-ins reduces ED visits, as well as hospital and SNF admissions, Dickson said.
Currently, UMass Memorial Health is providing MIH “for free,” he added. The UMass system absorbs the cost but that process is unsustainable. Dickson said “it makes no sense whatsoever” for an insurance company to pay tens of thousands for a patient travelling through an ED, hospital, or SNF, but to balk at the roughly $1,000 cost for mobile integrated health.
Apply for the 2027 AHA Foster G. McGaw Prize
The American Hospital Association is now accepting nominations for its prestigious 2027 Foster G. McGaw Prize, which recognizes organizations that improve community health and wellbeing through leadership and community partnerships. Honorees forge effective collaborations with a broad range of community organizations to improve access to care and address societal factors influencing health. Past award winners have co-created mental health crisis clinics, expanded housing options to help people transition out of homelessness, and used strategic investments to expand capacity in vital community benefit organizations. This annual award honors one winner and up to three finalists, which will be recognized at the 2026 AHA Leadership Summit in Denver. AHA is accepting applications through May 5. Cambridge Hospital (1993), Massachusetts General Hospital (2015), and Boston Medical Center (2024) were previous winners, while MGH, Baystate Health, and UMass Memorial Medical Center (three times) have been among the past finalists.
District Court Rules Against Leapfrog Methodology
A federal judge has ruled that the Leapfrog Group, one of the major hospital rating services, unfairly graded hospitals that failed to participate in the survey that Leapfrog uses to calculate patient safety. Leapfrog was ordered to remove the grades it assigned to five Tenet Healthcare hospitals in Florida that brought suit against it and to send notices to all hospitals that paid to license recent safety grades saying that those grades “were found to be deceptive and unfair.” The United States District Court also ordered Leapfrog to cease assigning grades under any methodology that scores non-participating hospitals differently than participating hospitals. Leapfrog immediately announced it would appeal the ruling.
Participating in Leapfrog surveys is purely voluntarily. If a hospital does not participate, Leapfrog uses other “imputed” methods to generate its safety score, and in 2024 it changed that imputed methodology. The judge found that “Leapfrog’s change in methodology has no scientific basis, unfairly penalizes nonparticipating hospitals, and misrepresents hospital safety.”
Round Two of Connected & Online Program Begins
The Massachusetts Broadband Institute (MBI) has launched the second round of its $28.5 million “Connected & Online Program,” which is meant to provide more than 32,000 internet-enabled devices to eligible organizations across Massachusetts.
Organizations, including healthcare providers, can apply to receive the devices for use in advancing education, workforce development, and healthcare access under one project. Those requesting devices must use them to increase access by establishing public device lending programs and on-site device stations. Devices will be fully loaded with software, selected accessories, and warranties at no cost to awardees. The application deadline closes at midnight on Sunday, April 5, and awardees will be notified in early May.