
INSIDE THE ISSUE
> Premium Tax Credits
> Rural Hospital Funding
> Healthcare Worker Vaccinations
> Cybersecurity Threat Reporting
> Transition at DMH
MONDAY REPORT
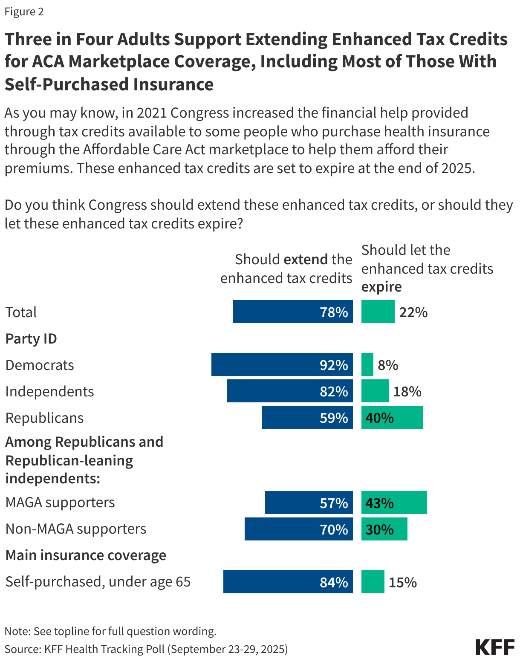
Polling Supports Extending Enhanced Premium Tax Credits
The federal government shutdown last week centered mainly on the dispute between Democrats and Republicans over extending enhanced tax credits for people who buy their own insurance through the Affordable Care Act marketplace. The credits are set to expire in December and without an extension, premiums are expected to increase significantly. Democrats want them included in the continuing resolution that passed the Republican-controlled House of Representatives and that was sent to the Senate, but GOP leadership and the White House refused.
A KFF poll released on Friday found that 78% of adults say Congress should extend the credits. The support crossed party lines with 92% of Democrats, 82% of independents, 59% of Republicans endorsing the extensions. Republicans who align with the MAGA movement (57%) also say Congress should extend these subsidies, according to the poll.
The Massachusetts Health Connector says that if the enhanced premium tax credits are not extended, more than 337,000 residents of the commonwealth will see increased healthcare costs in addition to the increase in premiums during open enrollment that have already been announced by health plans facing record losses.
“Massachusetts families should never have to choose between putting food on the table and keeping their health care coverage,” said Massachusetts Congresswoman Lori Trahan (D) last week in a media release featuring the Connector’s projections. “But that’s exactly what will happen if President Trump and Congressional Republicans refuse to act. The data is clear: costs are skyrocketing, hundreds of thousands of Bay Staters are at risk of losing coverage, and families are already receiving notices warning them of higher premiums before open enrollment even begins.”
Last week, due to the shutdown and the immediate cessation of certain health programs, hospitals in Massachusetts were required to move patients receiving inpatient care through innovative “hospital-at-home” programs out of their homes and back into brick-and-mortar hospitals.
On September 27, HHS and its operating divisions released their FY 2026 contingency plans, which describe staff to be furloughed, how specific programs will be affected, and other pertinent details. HHS estimates that 47,257 employees will be retained while 32,460 will be furloughed. The Centers for Medicare and Medicaid Services and the Health Resources and Services Administration within HHS are each expected to retain 53% of their respective workforces. But unlike previous shutdown protocols, which typically involved temporary furloughs with reinstatement upon the resumption of funding, the administration is encouraging agencies to consider reduction in force (RIF) notices for employees in programs that lack discretionary funding or are not aligned with current administration priorities. Unions representing federal workers filed suit last Tuesday saying that using a lapse in appropriations as a ground for eliminating programs and jobs is illegal.
While Finances and Coverage Struggle, State Seeks Federal Funding
In addition to the news about the shutdown, last week also saw State Revenue Commissioner Geoffrey Snyder announce that federal tax code changes in the One Big Beautiful Bill Act (OB3) will reduce Massachusetts tax revenues in FY2026 by more than $650 million. OB3 is also projected to result in at least another 250,000 people losing health coverage in coming years, placing further stress on the Health Safety Net and hospital finances.
Amid the cascading bad news, the state announced that it is pursuing funding from a positive part of OB3 – the $50 billion appropriated to rural hospitals. The $50 billion Rural Health Transformation Program invests in rural providers from FY2026 to FY2030. The Massachusetts Executive Office of Health & Human Services (EOHHS) released a notice of its intent to submit a grant application on behalf of Massachusetts and also issued a Request for Information from interested parties on how to improve rural healthcare access, quality, and outcomes; the state will use this info as it drafts its application for the grant funding.
State applications for a piece of the funding must be submitted by November 5, 2025. The Centers for Medicare and Medicaid Services will determine state award recipients by December 31.
DPH to Hospitals: Healthcare Workers Must Receive Flu & COVID-19 Vaxs
Last Tuesday, the Department of Public Health (DPH) released guidance to hospitals on the requirements to vaccinate healthcare personnel for flu and COVID-19, and the need for hospitals to report vaccination rates to DPH as they have in previous years.
The notice reads, “Based on clinical evidence and in alignment with the Northeast Public Health Collaborative and CDC recommendations, being up to date with vaccine doses for COVID-19 means that all HCP must receive one 2025-2026 COVID-19 vaccine,” unless the individual is exempt from vaccination.
The Northeast Public Health Collaborative, of which DPH is a member, “is a voluntary coalition of regional public health agencies and leaders, brought together to share expertise, improve coordination, enhance capacity, strengthen regional readiness, and protect evidence-based public health.” It was formed in September.
DPH defines “healthcare personnel” as “any individual or individuals who either work at or come to the licensed hospital and who are employed by or affiliated with the hospital, whether directly, by contract with another entity, or as an independent contractor, paid or unpaid including, but not limited to, employees, members of the medical staff, contract employees or staff, students, and volunteers, whether or not such individual(s) provide direct care.”
Healthcare personnel who are not exempt must receive a 2025-2026 COVID-19 vaccine and a seasonal influenza vaccine no later than March 31, 2026. Hospitals may require that exempt personnel take mitigation measures such as wearing facemasks during patient care encounters and avoiding direct patient care.
The DPH guidance released last week requires hospitals to track all flu and COVID-19 vaccinations, as well as exemptions, and report that data to DPH.
Law Protecting Liability for Cybersecurity Threat Info Sharing Lapses
On October 1, the Cybersecurity and Information Sharing Act (CISA) expired. CISA extended legal protection to organizations that voluntarily reported cybersecurity threats to the federal government, in an effort to encourage information sharing and strengthen security protocols. For hospitals, this generally entailed reporting threats that attempted to breach cybersecurity systems but failed. Successful breach reporting is, and continues to be, governed by the HIPAA Breach Notification Rule and the Cyber Incident Reporting for Critical Infrastructure Act (CIRCIA), both of which mandate reporting cybersecurity breaches under a specific set of guidelines.
There is broad interest in Washington for reauthorizing CISA. An extension of CISA is included in both parties’ temporary funding proposals, which have so far failed to pass, resulting in the shutdown. The U.S. Department of Homeland Security has stated it will continue to support functionality for the portal to report cybersecurity threats during the shutdown, although with CISA’s expiration it is unclear if the liability protections will be in place during this time.
Transition
Last Friday, Department of Mental Health Commissioner Brooke Doyle announced she is stepping down from the post, effective today. She has led DMH since 2020. Deputy Commissioner Beth Lucas will lead the agency on an interim basis until a new commissioner is named.
During her tenure, Doyle was instrumental in significant changes to the behavioral health system in Massachusetts, including the launch of the Behavioral Health Help Line and Community Behavioral Health Centers, the addition of hundreds of inpatient psychiatric beds at acute care hospitals and freestanding psychiatric facilities, and the growth of the behavioral health workforce. She also managed an overburdened DMH continuing care system and instituted pediatric behavioral health diversionary programs that have significantly reduced pediatric emergency department boarding.