Violence Prevention, Econ Development, and more …

INSIDE THE ISSUE
> The Senate’s Violence Prevention Bill
> Econ Development Bill
> Stuck Patients and Medicare Advantage
> 340B Developments
> Non-Profit Reporting Bill
MONDAY REPORT
Vote on Senate’s Violence Prevention Bill Expected This Week
The State Senate this week is expected to vote on its version of a workplace violence prevention bill that the House passed last year.
The end-of-the-session Senate action culminates a multi-year process to pass some form of worker protection legislation. While various proposals had been put forth in the past, the issue gained traction when MHA, the Massachusetts Nurses Association, and the Massachusetts Division of 1199SEIU collaborated on consensus legislation.
The House and Senate bills each require healthcare facilities to establish a standardized framework for violence prevention and response, create new state-level reporting procedures, and entitle victims to paid leave while seeking legal support following a violent incident. But they differ in one very important point: the House version maintains the misdemeanor charges for assault and battery against healthcare workers that is currently in statute but would add two additional graduated penalties. Assault and battery against healthcare workers – if done “knowingly and intentionally” by the perpetrator and results in victim bodily injury – would be able to be charged as a felony offense that could incur penalties of five to 10 years in prison, according to the House version. The Senate bill does not include felony language, but makes the misdemeanor charge an arrestable offense regardless of whether it was witnessed by law enforcement, allowing for immediate removal from healthcare facilities.
At a press conference last Thursday announcing the Senate action, the lead sponsor of the Senate bill, Sen. Joan Lovely (D-Salem), explained that the Senate language is similar to language currently on the books for domestic violence in that it allows warrantless arrests in situations where the officer has probable cause to believe the suspect committed the assault.
Among those speaking at last Thursday press conference was Liz Taranto, an ambulatory care nurse, who recounted the shocking details of being kicked and threatened with scissors while she treated patients. Shannan Bush, a nurse at Boston Medical Center, recounted similar physical and verbal assaults that occur on an almost daily basis, saying, “It’s not OK and it needs to stop.”
Speaking on behalf of MHA, Christi Barney, the vice president of quality and patient safety and chief health equity officer at Emerson Health, said, “It is our great privilege to take care of anyone who walks into any of our healthcare organizations. We know we are often meeting you at one of the most stressful points in your life. And yet, we can’t be the best we can be, do all that we need to do to take care of you if a part of us is always worried about the safety of ourselves, the safety of our team, and the safety of the people that are around us.” Barney is co-chair of MHA’s Healthcare Safety & Violence Prevention Workgroup that collected and published data to help define the problem, and issued guidelines for healthcare safety and violence prevention that hospitals have adopted.
The House and Senate bills, while enjoying the great support of nurses, are constructed to protect all staff working in healthcare facilities.
Econ Development Bill Could Further Help Health Safety Net
The $561 million economic development bill that the House passed last Wednesday and the Senate’s version that is scheduled for a vote this week contain a wide variety of initiatives touching nearly all sectors of the economy, including healthcare.
For example one provision of the bill that passed the House would rename the existing “Commonwealth Federal Matching and Debt Reduction Fund” to the “Commonwealth Federal Matching Fiscal Resilience Fund,” and includes language allowing money to be more easily transferred from it to hospitals, health centers, the Health Safety Net, among other potential recipients. Governor Maura Healey had first proposed this provision in her Discovery, Research and Innovation for a Vibrant Economy (DRIVE) legislation, portions of which are also incorporated in the economic development bill.
The recent FY2027 state budget that Healey signed last Thursday contains a $37.5 million transfer from the Commonwealth Federal Matching and Debt Reduction Fund to the Health Safety Net. MHA had advocated for this additional funding for the Health Safety Net in light of increased funding shortfalls in the program due to the loss of ConnectorCare coverage for 36,000 people in January 2026. The new language in the econ development bill would allow the Administration and Finance Secretary to make additional transfers as the commonwealth braces for hundreds of thousands of newly uninsured from Medicaid and the Connector due to new limitations called for in the One, Big, Beautiful Bill Act that takes full effect in FY2028.
Also potentially benefitting the Health Safety Net (which runs ever-increasing shortfalls borne solely by hospitals) is an “historical horse racing” amendment from Rep. Adrian Maduro (D-East Boston). Such horse races allow players to wager on electronic replays of past horse races using a pari-mutuel betting system. All identifying parts of the races (names of horses, jockeys, courses, etc.) are stripped out but other performance data and odds are kept in to allow people to bet. Maduro’s amendment which passed the House would dedicate a portion of the “take” to the Health Safety Net.
Throughput Concerns Focus on Medicare Advantage
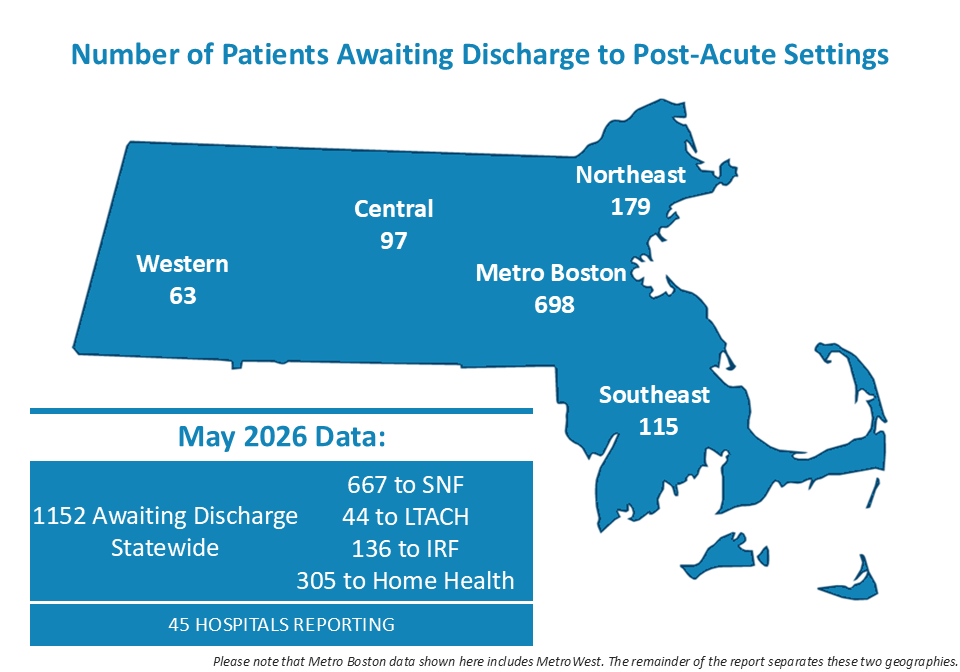
MHA’s latest throughput survey shows that in May approximately 1,152 patients were stuck in acute care hospital inpatient beds unable to transition to the next level of care – such as to a nursing home, rehab facility, or home healthcare setting.
The transfer of patients from one care setting to another has been a persistent problem, with the population of patients stuck in acute care hospitals sometimes exceeding 2,000 at any one time. The reasons for the backups are many, but according to hospital case managers that were surveyed the most commonly identified roadblock is insurance company administrative barriers – namely, the requirement that patients and providers receive prior authorization from the insurance company before a patient transfer occurs.
In its most recent report to Congress, the Medicare Payment Advisory Commission (MedPAC) presents evidence that backs the claims of case managers that responded to the MHA survey. MedPAC found that the increase in Medicare Advantage (MA) enrollees in recent years may not have affected hospital finances greatly, but Medicare Advantage policies have affected operations. Specifically, MedPAC’s interviews with post-acute care (PAC) providers revealed that “prior authorization is the most significant MA-related challenge they face.”
Inpatient rehab facilities (IRF) and skilled nursing facilities (SNF) “reported that MA plans were difficult to work with. Requests for prior authorization to admit enrollees and to extend stays were burdensome and costly to administer. SNF interviewees told us that even if the MA payment rates were close to [fee-for-service] rates, they found the process of authorization for longer stays for enrollees to be challenging and administratively costly. One SNF told us that it used to avoid MA given the administrative hassles and low rates … but that the growth in MA made this approach less tenable.”
Congressional Activity on 340B Picks Up Steam
In addition to the major reforms to 340B drug prices that the Centers for Medicare and Medicaid Services included in its calendar year 2027 hospital outpatient prospective payment system proposed rule, several members of Congress have taken action on 340B over the past few weeks.
In the House, a bipartisan group of Energy and Commerce Committee members, consisting of Reps. Scott Peters (D-Calif.), John Joyce (R-Penn.), Jake Auchincloss (D-Mass.), Dan Crenshaw (R-Tex.), and Nanette Barragán (D-Calif.), introduced the SECURE 340B Act (H.R. 9599) on July 6. While this bill would implement a four-year moratorium on the retrospective rebate model that U.S. Health & Human Services proposed in favor of a third-party clearinghouse, it would also place restrictions on qualifying patients and child sites and establish stronger audits and potential sanctions for participating hospitals.
“Employees’ health premiums are too high, and the growth of the 340B program is one driver of that inflation,” Auchincloss said.
In the Senate, Health, Education, Labor, and Pensions Committee Chair Bill Cassidy (R-La.) has released his own draft of legislation that would reform the 340B program. Relative to the House bill, this draft goes a step further, not only implementing considerable auditing processes and restricting patient eligibility and child site flexibilities, but also permitting drug manufacturers to choose to provide 340B rebates via a post-acquisition rebate.
Finally, in light of Eli Lilly’s ongoing termination of 340B prices for select entities not complying with the patient-level claims reporting policy it has implemented, a bipartisan group of 72 Representatives (61 Democrats and 11 Republicans) have sent a letter to HHS asking that it take action to end Eli Lilly’s policies regarding claims reporting and 340B price termination. From the Massachusetts delegation, Reps. Stephen Lynch, Jim McGovern, Seth Moulton, Ayanna Pressley, and Lori Trahan signed the letter.
Non-Profit Hospital Reporting Bill
Earlier this month, the U.S. House Committee on Ways and Means advanced the Tax Exempt Hospital Transparency Act (H.R. 9504) to the House floor by a vote split along party lines. This legislation would expand Internal Revenue Service reporting requirements for non-profit hospitals by requiring additional disclosures related to community benefit spending, subsidized service lines, financial assistance programs, and utilization of the 340B Drug Pricing Program. Larger non-profit hospital systems, defined as those with more than 100 staffed inpatient beds that are not critical access hospitals or rural emergency hospitals, would face additional reporting obligations aimed at increasing transparency surrounding the use of their tax-exempt status.
During the hearing, Democratic committee members, including Committee Ranking Member Richard Neal (D-Mass.), raised concerns that the proposal emphasizes duplicative compliance reporting rather than addressing the root causes of healthcare affordability, while Republican supporters argued that the bill would improve public accountability for tax-exempt hospitals.